On the task of siding with life
Lessons from a quarter of a century of “new euthanasia”
by Moritz Nestor

(Picture © imago / Gustavo Alabiso)
cc. The following article was written to mark the 20th anniversary of the founding of the “Hippocratic Society of Switzerland” – but the questions it raises revolve around core anthropological issues and are of fundamental importance. The article is about our attitude to life, to our fellow human beings, to the relationship of the generations with each other, as well as about placing these question in a socio-political context. They do not only provoke thoughts in connection with the repeatedly heated debate about euthanasia and assisted suicide, they are also highly topical against the background of the current discussions about an allegedly necessary “balancing of goods” between health and economy in connection with Covid-19.
Dear Ladies and Gentlemen
Allow me a personal preliminary remark. My father was an officer in the “Wehrmacht” of the “Third Reich”. He narrowly escaped death in 1943 during the rearguard action in the Chertkovo basin, shot in the head and with frostbitten feet. I grew up deeply affected by the war and also by Nazi euthanasia. My father, who after six years of war had to continue to kill in his dreams for thirty-five more years, until his death, is a warning example to me of what it means to no longer be able to come to rest in life, because one has been involved – actively or passively – in killing. And it is deeply disturbing to have to think one day about whether your beloved father killed with the same hands with which he caressed you.
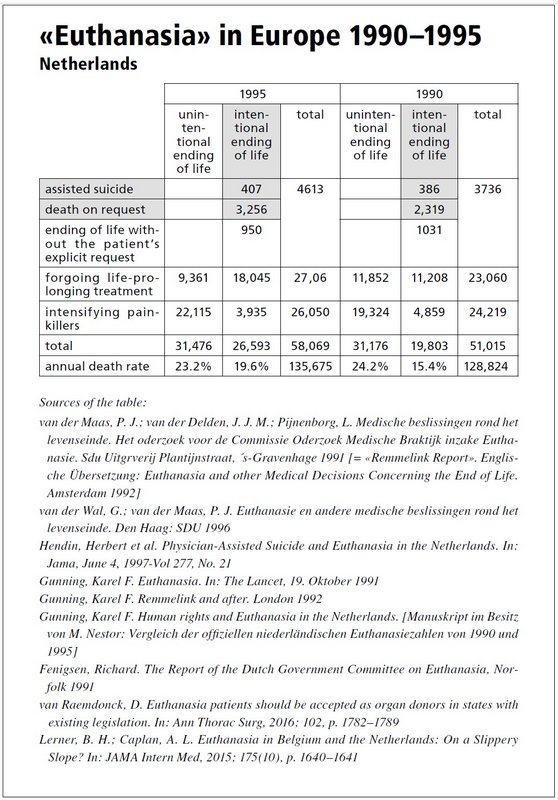
When I read the article “Uncharted ways of euthanasia in Holland”1 in the “Neue Zürcher Zeitung” of 29/30 May 1993, I was left in disbelief.2 In the democratic Switzerland of 1993, what were “uncharted” ways of euthanasia supposed to be? The NZZ article was the prelude to the campaign for the legalisation of “euthanasia” in Switzerland.3 At that time, we learned that the frightening example presented in the NZZ article was the result of a gradual liberalisation of patient killing in the Netherlands since the 1970s, which was now coming to Switzerland. In the governmental reports of the Netherlands we found the “euthanasia” figures for the years 1990 and 1995. 1990: 19,803 (out of 128,824 deaths in this year) and 1995: 26,593 (out of 135,675 deaths in this year).4
Public discourse about killing as if it were a form of “love”, and its consequences
At the core of the Hippocratic Oath lies the prohibition of killing. The oath is the oldest code of professional ethics known in human history. Its great age of over 2,500 years and the fact that in all that time no penal law was needed for it to hold among doctors reflects what Viktor von Weizsäcker, one of the founders of psychosomatic medicine and modern medical anthropology, wrote in his 1923 essay “Hippocrates and Paracelsus”: the doctor’s profession is, he says,
“an everlasting, perhaps eternal one. And as it is man’s eternal fate that we become ill and need help, so that is why the doctors’ actions have a history […]. But medicine does not come and go like a people, a culture, it is longer, its art is of long duration […], and this is precisely why it participates in everything that is longer than a story, why, like philosophy, it participates in the perpetual, the infinite – pertaining to the spirit. […] it does not originate in the spirit, but in life, in that cell of earthly existence with its pains and sufferings […] the “philosophos” [is] a lover of health or wholeness – thus basically a physician. For a gifted doctor will be […] he who has a sense of harmony, a sense of beauty, wholeness and perfection; he will feel all the more keenly what is needed, or what is lacking, the stronger his longing for the beautiful, the whole, the stronger his love for the ailing will grow out of his love for the healthy.”5
Have we not become doctors and psychotherapists because we were touched somewhere by that “love of the ailing” and that “love of the healthy” of which Weizsäcker speaks here, and through which, as he says, we “feel what is needed, or what is lacking”?: How does one become a doctor? Viktor von Weizsäcker answers the question “How do you become a doctor?” by means of a moving image:
“When a little sister sees her little brother in pain, she will find a way before all knowledge: fondling him, her hand finds the way, caressing, she wants to touch him where it hurts. So the little sister becomes the first doctor. A foreknowledge of a primordial effect prevails in her, even though she is unconscious of it: it guides her urge to the hand and leads the hand to the effective touch. For this is what the little brother will experience: the hand does him good. The sensation of being touched by the sisterly hand comes between him and his pain, and the pain retreats before this new sensation. And this is the genesis of the first concept of a doctor; so the first technique of therapy comes into being. In fact, here, being a doctor is entirely in the small hand, being ill is entirely in the aching limb, and it will always remain so; even if the hand grows larger and arms itself with instruments or lends its strength to healing poisons or the speaking mouth, it will always remain, this hand, equally skilled in touching and taking hold, in caressing and cooling, an essence also of later medical activity.”6
“With the question: What is the trouble? [...] the primal phenomenon of being a doctor is introduced into reality. This everyday occurrence [of the ailing person’s encounter with his doctor, MN] deserves to be regarded with earnestness, yes, even solemnity.”7 Its “beginning [is] not knowledge, but asking questions.”8
So now, in 1993, the new “euthanasia” campaign also began in Switzerland. In autumn 1993, a member of the Dutch Society for “Voluntary Euthanasia”, Piet Admiraal, appeared in the Aula Magna of the University Hospital of Zurich for the first time. The co-lecture was given by a Dutch opponent of euthanasia, Prof. W. C. M. W. Klijn, Professor of Ethics at the University of Utrecht and member of the “State Commission on Euthanasia” in the Netherlands, who warned us urgently: “You have Article 115. It will become the gateway.”
Since then, the country has been inundated with euthanasia propaganda, and, in the last ten years, as aggressively as never before and to an extent that can hardly be surpassed. It was people like the philosopher Robert Spaemann, the psychiatrist Klaus Dörner and, above all, the German disability and hospice groups, who had realised even earlier that as little as only simply talking publicly about killing will cause serious social harm. When it was claimed that “being allowed” to talk about “euthanasia” was a question of tolerance, Spaemann was fond of quoting Aristotle: “Whoever says that it is allowed to kill one’s mother deserves not arguments but rebuke.”9 We only gradually understood what he meant back then. And what I am saying now is the lesson of thirty years of history.
The seriously ailing person is always existentially dependent on appropriate medical help and on the compassionate care of his relatives, good friends, doctors and nurses, who not only “care for” him, but support him compassionately, tirelessly instilling courage, confidence and hope. If the social environment, especially also doctors and nurses, radiates the ethos that everything humanly possible will be done to alleviate suffering, to heal; to do what is possible, and in the most difficult hours, where medical skills reach their limits, not to abandon the sick person, but to go through the most difficult times together – then such compassionate support is decisive for the course of the disease to a degree that should not be underestimated. The will to live and the hope for recovery play the most important role in the course of the disease and for the chances of recovery, in addition to the best possible medical treatment. This inner strength must be instilled in the despondent patient by his fellow human beings. The dependence of mortality on social connectedness is well documented in science: Thure von Uexküll summarises several studies in his standard work “Psychosomatics”: People with
“the least social ties and human relations showed a mortality 2.3 times (for men) and 2.8 times (for women) higher than the group with pronounced social ties and human relations. […] [and that, MN] unaffected by health status at the time of the start of the study and the year of death, socioeconomic status, health-damaging behaviour […] as well as physical activity and use of preventive health services.”10
In the past, the drama of suicide was not done justice when it was demonised as a sin. But neither is it done justice today when it is glorified as “self-determination”, altruistic compassion or even an act of love. But this is exactly what has been propagated since 1993.
Erwin Ringel, the father of suicide research and a student of Alfred Adler, warned that suicide is neither a sin nor an act of self-determination.11 The motive for suicide is rather a deep human need that must be recognised. The doctor, but also all others involved, must learn to understand the psychological drama behind the desire for suicide and what has gone before this, when a person’s own death appears to be the only possible way out.12
This “mental constriction” (Ringel) can occur especially in people who find it difficult to cope with being dependent on care. Having to accept help can trigger such strong emotions of self-rejection in them that at length, they feel worthless and a burden for their fellow human beings, until suicidal thoughts suppress any positive relationship to life – if the human environment cannot counteract this.
This process is artificially taken up and reinforced by public talk about killing as an alleged choice, as an “autonomous” decision, as a “labour of love”. In the resulting social climate, old and sick people in particular begin to feel that they are a burden on family and society. At some point, the gradual inner erosion of their self-worth is so advanced that they begin to feel morally obliged to talk to their spouse, relatives or doctor about “euthanasia” and even to “desire” being killed.
Human life, especially in its first and last phase, is fragile and highly dependent on support and help. This is a fact seldom realised by capable people in their healthy days, who throughout their lives have drawn their significance for their fellow human beings from the fact that they were strong, independent and willing to help. The realisation that their usual strength is suddenly diminished by ageing or illness and that they can no longer cope with everything as quickly and powerfully as they used to, often shakes their self-confidence. It is especially difficult for them to accept help when nature sets previously unknown limits to their hard-working lifestyle, which was a blessing for relatives and fellow human beings, and which can no longer be overcome by their will. Whole areas of previous life activity break away.
A lifestyle focussed on efficiency is not the only, but the most important factor obscuring sick people’s view of their rich life experience, which enables them to take a mature overview of what it means to have lived a whole life span. This is not possible for young people at the beginning of their lives. The elderly are living witnesses of the past and contribute to the fact that cultural development does not stop. Their overview gives rise to the wisdom of old age, on which the younger generation in particular can rely, so as to have their small and large worries weighed more calmly by the more realistic view of old persons with their experience of life.
It is a great fellow-human task to encourage people in this situation with so much courage and realism that they will be able to reconcile themselves to their weakness, that they will be able to plan more perseveringly, calmly and realistically and possibly conquer hitherto unrecognised areas of life – namely precisely also their above-mentioned significance for the first generation, which is still staggering at the beginning of life. This, too, is part of human freedom.
The ailing and those in need of help may become despondent, may doubt the meaning of life and no longer feel the strength to go on living, especially when they are suffering from pain. If a doctor or relatives or media products interpret this lack of strength and courage as an expression of a “free decision” to kill oneself, then the sufferer is cut off from help to master his difficult situation together with others. He feels abandoned, which will all the more encourage suicidal thoughts.
We humans owe our lives to the generation of our parents and grandparents, as it was their gift to us. It was their help and care that enabled us to become human. Therefore everyone feels a deep obligation of gratitude and so wants to return to them today what they have once given us – given out of love, without our even asking for it. This invisible contract binds the generations together naturally. It forms the core of our social nature.13 Just as we were as children, so today the old generation is entitled to the same full commitment and loving care that we once gladly received from them. This is the natural right of the generation of parents who have grown old. This inter-generational contract is irrevocable.14 We can violate it, but a person’s “mistaken opinion about himself and about the tasks of life sooner or later comes up against the sharp protest of reality, which demands solutions in the sense of community spirit”15, since, without mutual help, human coexistence becomes impossible. “What happens when this clash with reality takes place, can be likened to a shock effect,” Adler notes: the fellow human damage is an accusatory expression of the denied right to help.
The concern for success and for the protection of life accompanies us throughout life, especially in illness and helplessness in old age – even if digital automation as well as prosperity cloud our view in ths respect. Those who help others become more certain that they too will be helped in difficult situations. This creates a sense of security and trust that can alleviate the fear, to which we humans are so prone, and make life bearable. That is the best possible protection of life.16
It is precisely people who are able to accept help and have thus courageously overcome a serious illness or need for help, that convey courage to others and the hope that the latter can and will also be helped in difficult hours. Through the public talk about “euthanasia”, however, the ailing and those in great need of help experience that their fellow human beings, on whom they depend and from whom help might come, consider death as a solution. The ailing person is abandoned to fear. This emotionally weakens him, and also all others involved. The natural compassion and the spontaneous innate impulse to help, which the child already expresses in the first year of life without having to be taught, which is part of its nature, is weakened, disintegrates. At some point, the euthanasia society reproaches that doctor who still wants to help, for wanting to prevent a desperate sufferer from dying. In a society where the natural impulse to want to help comes to a standstill, the strength and hope to overcome difficult tasks and to grow in doing this slacken everywhere.
Thus, alone the talk about and the constant media coverage of killing out of compassion work against the basic conditions of human life. Human emotional connectedness and natural compassion are twisted into “deadly compassion”. The natural social forces of the human being, as we know them from the rich findings of anthropology, individual psychology and developmental psychology, the human sense of solidarity and community atrophy in the individual and in society, when they are exposed to this social psychological operation.
Since everyone gets sick at some time, public talk about “good killing” hits first and foremost the protective sphere of the family and the patient’s relationship of trust with his doctor, the guardian of life. But when the doctor is publicly said to be responsible for the “good death” and to be able to “unselfishly” deliver the patient for “love”, then the doctor becomes a danger. I will no longer be able to trust that I can turn to the doctor without fear, that everything he does is for my good, and that I can be sure that he is and remains the guarantor of my will to live – this trust will be destroyed.
We have seen honestly written reports from many countries about the true processes of “euthanasia”, which the public never learns about from the media products of the euthanasia debate talking about the “good death”. In these reports, relatives relate of their realisation after the act that they have become an accomplice, and guilty of the death of a beloved relative, how they become depressed and wonder, burdened with shame, how they are now to go on with their life.17 The images of euthanasia doctors with their petrified and mechanical reactions after a patient killing are also well-known, and suggest why these doctors had to go for a weekend of withdrawal after an “assisted suicide”.18
Public talk about killing is already a disposal of human life, that will at some time somewhere lead to acts against life, and that will destroy basic moral attitudes. If there is a public “debate” that it is a “deed of love” to give poison to people whose lives are no longer considered worth living, then this judgement is a heteronomy and thus a disposal of the life of a patient. In a social climate characterised by this, anyone can become an accomplice simply by silent acceptance. This is because silence has the same effect as acquiescence.
Because of their profession, doctors and psychologists are advocates of life. They know what public talk about killing does to the soul of patients. And they also know, above all, what happens in the inner life of people who actively or “passively” participate in the killing of their patients or family members. Anyone who gives poison to a person tired of living has previously made a value decision. He evaluates the life of the other person as no longer worth living. So, in reality, the suicidal person dies heteronomous.
Doctors and psychologists can assess what will be the consequences for society in the long run of such processes, in which people decide on the value of the lives of others. For this reason, they bear a special responsibility towards society, namely to inform it about what the influence of the continuous flood of films, talk shows and other mass propaganda about “euthanasia” will be on society as a whole: social bonds and solidarity between people, as well as all the interpersonal strength of which humans are capable, will slowly be weakened in all areas. The medical ethicist Giovanni Maio describes this “lentiprocess” in society as a whole, which remains unnoticed, while dangerously shifting basic ideological attitudes towards life in all minds:
“A society that does not view suicide with dismay, but declares it to be an understandable act, runs the risk of also sending other people to their deaths, because in this way it is signaled that our society can understand suicide, and even considers it reasonable. A society that considers it reasonable to take your own life in the face of illness is dangerous. For it will drive into even deeper despair many people, who are struggling with themselves and despairing about whether their life is still worthwhile and whether they are not just a burden”.19
When the euthanasia campaign began in 1993, it was part of a restructuring of the Swiss state according to the US-American concept of New Public Management: “Rethinking the state” meant running the state like an office with management methods. This included, in parallel with the euthanasia campaign, the conversion of state hospitals into profitable enterprises. The “new medicine” that has now been introduced is characterised as follows in “Careum working paper No. 2/2009”.
“Future viability requires a fundamental change in the therapeutic relationship. The individual doctor-therapist relationship is normalised to the extent that it […] basically follows the laws of the world of goods and consumption. […]. The “new medicine” is […] a cost-intensive mass market with high demand and increasing specialisation and division of labour. In the perception of the consumer, the comparison of services is important and there is competition between providers. Transparency is therefore an indispensable prerequisite, especially for the protection of patients. In highly standardised care, it is not a question of craft or art, but of comprehensible service descriptions. Accordingly, a therapeutic relationship based on an individualistic conception and clinical purism is obsolete.”20
Immediately after the fall of the Iron Curtain and the collapse of the Eastern Bloc, we witnessed the onset of the campaign to legalise drug use; it gave rise to the open drug scene on the Platzspitz and the Letten in Zurich and to its consequences. At the same time the restructuring of the education system was entered upon, and a little later began the “reform” of nursing education according to the same concepts. We encountered the same ideological concepts, actors and foundations in all areas. Ernst Buschor, for example, joined the Department of Education after the restructuring of the Zurich hospital system.
In the early years, resistance to the euthanasia campaign was at the forefront of our activities. From 1993/94 to 2000, we resisted the campaign to “liberalise” Article 114 of the Swiss Penal Code, which sanctions homicide at the request of the victim. Then, by an overwhelming majority, Parliament stopped the legislative initiative of Social Democratic leader Franco Cavalli to introduce “active assistance of euthanasia”, based on the model of the Netherlands. Today we can look back with great pride at this success, to which the Hippocratic Society contributed very energetically and significantly. We saw at that time that the front of the anti-“euthanasia” movement ran across all political camps and the right-left schema, and we found, across all ideological and religious differences, allies and loyal comrades-in-arms who were aware of the long-term consequences for a society when the state no longer provides the protective framework of legal equality.21
Equality of rights
The rule of law rests on the fundamental idea passed on to us from Greek antiquity: peace must be a just, a secure peace. Man must use his reason and, guided by compassionate feeling, must relate the law in his state to a pre-state standard, to the nature of man, and adapt it to this. In this way, political action approaches justice. From this sprang, and interestingly enough this happened in parallel with the history of the Hippocratic Oath, the history of the emergence of the democratic constitutional state, which also lasted 2,500 years. In its modern form, with its monopoly on the use of force, it was and is the historical alternative to the struggle of all against all, to despotism, anarchy, the law of the jungle and the law of the strongest – to power politics of every hue. The “civil state” is equality under the law, which can overcome the class divisions of the 19th and 20th centuries as well as the religious divisions and the feudal order of earlier centuries.
The basic experience of man in the state of war of all against all is the fear of being killed. The means of overcoming citizens’ fear of being killed by their fellow citizens was the monopoly of all power in the hands of the state, which is bound by the separation of powers, by law and order and human rights and “whose power is superior to any other power and which is therefore capable of keeping in check the violence that private individuals use against one another, of restraining the horrors they inflict on one another by the super-horror that emanates from it.”22 The enemies of the war of all against all “agree to surrender their weapons to the state in order to remove the mutual threat, to use the state as a guarantor of their security against each other and to submit to it. [...] people no longer can and no longer want to settle their conflicts with their fists. Renunciation of violence and (legal) obedience make up the citizen.”23
Thus, in the early European modern era, we see “the birth of the modern state out of the sufferings of the civil wars of the 16th and 17th centuries”. It “is the institutional overcoming of civil war. It establishes civil peace by establishing the monopoly of legitimate physical violence and depriving citizens of the right and the power to be judges and bailiffs on their own account.”24 And yet this is the essence of euthanasia, that the “angel of death” presumes to be “judge and bailiff on his own account”.
The state order of peace knows no worse evil than death. Its purpose is the protection of life, physical integrity and freedom.25 In the protective state, all professions are called upon to fulfil the state’s purpose, the protection of life. However, this state can in turn become the object of citizens’ fear if it deviates from its purpose. This is the relevance of human rights. They are meant to protect the citizen against an overbearing state.
This model of the state is a fragile entity that must be lived consciously and, moreover, is only imperfectly developed in today’s states. “And yet political thought has not yet found a way back behind it without sliding into chaos.”26 These legal-philosophical considerations and the social-psychological ones are two sides of the same coin. Let us therefore go back for a moment: whoever decides to give poison to another human being has first made a value judgement: This life there in front of me is without any value. Otherwise, he does not even provide the poison, but soothes, helps and accompanies his fellow human being, even in his most difficult hour. This would be self-determination based on humanity, and this is what man needs “until his last breath” and must have, for cogent reasons. The “assistant to suicide”, however, wants a “self-determination that brings forth the last breath”.27
So how did it come about that in the only direct democracy in the world, of all places, the killing of ailing persons was put up for grabs and the equality of rights was abandoned, which took away people’s fear of their fellow human beings, especially of the doctor? Why did the Swiss “euthanasia” debate begin at the same time as the introduction of New Public Management? Is it mere coincidence that at the World Economic Forum 2000, the leaders of the Western industrial nations and high finance, representatives of the World Bank, the IMF and global investors discussed, together with the “euthanasia” philosopher Peter Singer, how much to spend on health in the future? At a time when the world was again arming itself and preparing for wars to come – as it is still doing! The attempt to introduce “euthanasia” is the implementation of what was planned there. I only wanted to hint at these connections briefly. They are a topic of their own.
After more than twenty-five years, the mental defences have been damaged in many parts of society. The task has become more difficult – but it remains the same: as guarantor of the ailing person’s life and as guarantor of the purpose of the state, to shed light upon processes that threaten the protection of life, whenever they are looming in the state. Recently, there has been a budding return to the Conditio humana: firstly, that “human autonomy is always autonomy in relationship (‘self-determination needs the other person’28)”. Secondly, the term “balance suicide”, coined by the psychiatrist Alfred Hoche in 1918 as a deliberate free will act of a healthy person29, which has been reused by the new euthanasia movement since the 1970s, remains very controversial among psychiatrists30, and gerontologists and gerontopsychiatrists are again urgently warning against it.31 The new “counter-proposals for a [...] new culture of care [...] should be urgently discussed”.32 Thirdly, the dubious hope that cruel suicides would be “transformed” into assisted suicides by allowing euthanasia is dashed by bitter reality.33 We know the “social contagion” effected by real and fictitious suicidal behaviour (“Werther effect”).34 Copycat acts can be prevented!35 Reporting can “prevent suicides if it reports on suicidal persons who found ways out of their emergency situation and were able to overcome their suicidality”.36
Sufficiently for what Ernst Bloch once called “docta spes”, the “taught hope”. •
1 The Dutch medical society KNMG and the governmental papers in the Netherlands officially use the term “euthanasia”, which was also used by the National Socialists: “Euthanasia is defined as the active termination of life at a patient’s voluntary and well-informed request.” [KNMG. Euthanasia in the Netherlands. 16.8.2017. https://www.knmg.nl/actualiteit-opinie/nieuws/nieuwsbericht/euthanasia-in-the-netherlands.htm (accessed 3 March 2019)] Noteworthy: In the official Dutch texts, “assisted suicide” is referred to as “euthanasia”, and according to the above definition is an “active termination of life”, thus a killing!
2 See also: Freispruch für ärztliche Hilfe zur Selbsttötung (Acquittal for medical assistance in suicide.) In: Neue Zürcher Zeitung, 1 October 1993
3 There are serious historical reservations about the term “euthanasia”, “because the National Socialist “euthanasia” law – which ultimately did not come into force – had the term in its title: “Gesetz über die Sterbehilfe bei unheilbar Kranken” (Law on euthanasia for incurable ill patients). In: Nestor, Karen et al. Hilfe beim Sterben, Hilfe zum Sterben oder Hilfe zum Leben? (Help in Dying, Help to Die or Help to Live?) In: Swiss Medical Forum - Schweizerisches Medizin-Forum 2017; 17(35), pp. 738–743, p. 738. The text of the proposed Nazi law of 1940 can be found in: Roth, Karl Heinz (ed.). Erfassung zur Vernichtung. (Collection for destruction), Berlin 1984. p. 177, see also: pp. 121, 130f., 143.
4 Cf.: van der Maas, P. J.; van der Delden, J. J. M.; Pijnenborg, L. Medische beslissingen rond het levenseinde. Het oderzoek voor de Commissie Oderzoek Medische Braktijk inzake Euthanasie. Sdu Uitgrverij Plantijnstraat, ’s-Gravenhage 1991. ISBN 90 39 901244 [= “Remmelink Report”. English translation: Euthanasia and other Medical Decisions Concerning the End of Life. Amsterdam 1992] See also: van der Wal, G. & van der Maas, P. J. Euthanasie en andere medische beslissingen rond het levenseinde (Euthanasia and other end-of-life medical decisions). The Hague: SDU 1996. See also: Gunning, Karel F. Human rights and Euthanasia in the Netherlands. [Manuscript in the possession of the author: Comparison of the official non-language euthanasia ceremonies of 1990 and 1995] See also: Fenigsen, Richard. The Report of the Dutch Government Committee on Euthanasia, Norfolk 1991.
5 von Weizsäcker, Viktor. Arzt und Kranker (Doctor and patient) I. 3. expanded edition. Stuttgart 1949, p. 7ff.
6 Ibid., p. 89
7 Ibid., p. 86
8 Ibid.
9 Spaemann, Robert. In: Stettberger, Herbert (Ed.). Berlin 2017, pp. 197–208, p. 202
10 Cf.: von Uexküll, Thure. “Psychosomatik” (Psychosomatics.) Quoted from: Eser, Albin (ed.). Lexikon Medizin, Ethik, Recht. (Encyclopaedia Medicine, Ethics, Law.) Freiburg/Br. 1992; Holt-Lunstad, Julianne. Testimony before the US Senate Aging Committee. 27 April 2017. [https://www.aging.senate.gov/imo/media/doc/SCA_Holt_04_27_17.pdf (accessed May 16, 2019)]; Holt-Lunstad, Julianne et al. “Social Relationships and Mortality Risk: A Meta-analytic Review”. In: PLoS Med 7(7) 2010: e1000316 [https://journals.plos.org/plosmedicine/article/file?id=10.1371/journal.pmed.1000316&type=printable (accessed 16 May 2019)] Maio, Giovanni. “Die heilende Kraft der Zuwendung in der Medizin”. (The healing power of caring in medicine). In: Ehm, Simone; Giebel, Astrid; Lilie, Ulrich; Prönneke, Rainer (eds.). Geistesgegenwärtig behandeln. Existentielle Kommunikation, Spiritualität und Selbstsorge in der ärztlichen Praxis. (Mindful treatment. Existential communication, spirituality and self-care in medical practice). Neukirchen 2016, pp. 57-70; Id. “Die heilende Kraft der Begegnung” (The healing power of encounter). In: Zeitschrift für Komplementärmedizin 2013, 5; 5, pp. 58-62; id. “Therapie als Hilfe zur Annahme seiner selbst: Über die heilsame Kraft der Begegnung”. (Therapy as help to accept oneself: On the healing power of encounter). In: Balint-Journal 2013. 14; 2, pp. 33-39.
11 Cf. Ringel, Erwin. Der Selbstmord. Abschluss einer krankhaften Entwicklung. (The suicide. Conclusion of a pathological development.) Wien/Düsseldorf, 1953
12 Cf.: Ringel, Erwin. “Das präsuizidale Syndrom – medizinische, soziale und psychohygienische Konsequenzen”. (The presuicidal syndrome – medical, social and psycho-hygienic consequences.) In: Hexagon “Roche”. 1985; 13(1), p. 8–14
13 Cf: Dührssen, Annemarie. Die biographische Anamnese unter tiefenpsychologischem Aspekt. (The biographical anamnesis from a depth psychological point of view.), Göttingen 1981. Cf. also: Nestor, Moritz; Vögeli, Erika. Zum Dreigenerationenmodell. (On the three-generation model.) 1998, https://naturrecht.ch/wp-content/uploads/1998-MZE-Erika-Moritz-Dreigenerationenmodell.pdf (accessed on 7 March 2019). Cf. also: Nestor, Moritz. 13 Thesen: Anthropologische Grundlagen der Familie (13 Principles: Anthropological foundations of the family.), 1999. https://naturrecht.ch/13-thesen-anthropologische-grundlagen-der-familie/ (accessed on 10 March 2019), cf. also: Nestor, Moritz. “Worin besteht der Sinn des Alters” (What is the meaning of old age?) 1997. https://naturrecht.ch/worin-besteht-der-sinn-des-alters/ (accessed on 10 March 2019), Guardini, Romano. Die Lebensalter. Ihre ethische und pädagogische Bedeutung. (The ages of life. Their ethical and pedagogical significance). Würzburg 1953
14 Cf. also: Nestor, Moritz. “In schwierigen Zeiten einen menschlichen Standpunkt gewinnen. Was uns geschichtliche Erfahrung, Naturrecht, Anthropologie und Psychologie dazu zu sagen haben – eine Annäherung”. (On gaining a humane stance in paltry times. What historical experience, natural law, anthropology, and psychology have to say – an approximation). In: Current Concerns No. 12 of 30 May 2017
15 Cf.: Chapter “Die Meinung über sich und über die Welt” (The opinion about oneself and about the world), in: Adler, Alfred. Sinn des Lebens (Meaning of Life). Leipzig 1933
16 Cf.: Chapter “Der anthropologische Aspekt: Gemeinschaftsgefühl als ursprüngliche Gegebenheit.” (The Anthropological Aspect: Sense of Community as an Original Condition). In: Kaiser, Annemarie. Das Gemeinschaftsgefühl bei Alfred Adler. Ein Vergleich mit Befunden aus Entwicklungspsychologie, Psychopathologie und Neopsychoanalyse. (Alfred Adler’s feeling of community. A Comparison with Findings from Developmental Psychology, Psychopathology and Neopsychoanalysis). Dissertation at the Faculty of Philosophy I of the University of Zurich 1977, p. 12ff.
17 Cf. Marker, Rita. Deadly Compassion: The Death of Ann Humphry and the Truth about Euthanasia. Morrow/Harper/Collins/Kirkus 1993. Cf. also: Müller-Frank, Stefanie. Sterbehilfe. “Die Fragen der Angehörigen”. (Assisted suicide. The questions of the relatives.) In: Deutschlandfunk Kultur of 13 February 2017. https://www.deutschlandfunkkultur.de/sterbehilfe-die-fragen-der-angehoerigen.976.de.html?dram:article_id=378852 (accessed on 3 March 2019).
18 Cf. IKON. Tod auf Verlangen. (Death on demand.) Television film. Netherlands 1994. Cf. also: Goddar, Jeannette. “Tod auf Verlangen”. (Death on Demand). In: TAZ of 12 December 1994. (http://www.taz.de/!1529588/ (accessed on 3 March 2019))
19 Maio, Giovanni. Medizin ohne Mass? (Medicine without measure?) Stuttgart 2014, p. 175
20 Panfil, Eva Maria; Sottas, Beat. Careum working paper 2. Woher kommen die Besten? Globaler Wettbewerb in der Ausbildung – wer bildet zukunftsfähige Health Professionals aus? (Where do the best come from? Global competition in education – who trains future-proof health professionals?) Careum 2009, p. 8
21 Bastian, Till (ed.). Denken, schreiben, töten. Zur neuen Euthanasie-Diskussion und zur Philosophie Peter Singers (Thinking, writing, killing. On the new euthanasia discussion and the philosophy of Peter Singer), Stuttgart 2000. Fenigsen, Richard. The Report of the Dutch Government Committee on Euthanasia, Norfolk 1991. Dörner, Klaus. Tödliches Mitleid (Lethal compassion), Freiburg/Basel/Wien 1993. Ib. Leben und sterben, wo ich hingehöre (Live and die where I belong). 5th edition, Neumünster 2007. Spaemann, Robert; Hohendorf, Gerrit; Oduncu, Fuat S. Vom guten Sterben. Warum es keinen assistierten Tod geben darf (On dying well. Why there should be no assisted death), Freiburg/Basel/Wien 2015. Ib. & Fuchs, Thomas. Töten oder sterben lassen? (Kill or let die), Freiburg/Br. 1997. Hoffmann, Thomas; Knaup, Marcus (eds.). Was heisst in Würde sterben. Wider die Normalisierung des Tötens (What does it mean to die with dignity. Against the normalization of killing), Wiesbaden 2015. Krause Landt, Andreas. Wir sollen sterben wollen. Warum die Mitwirkung am Suizid verboten werden muss (We should want to die. Why assisted suicide must be banned). Bauer, Axel W. Todes Helfer. Warum der Staat mit dem neuen Paragraphen 217 StGB die Mitwirkung am Suizid fördern will (Why the state wants to promote assisted suicide with the new paragraph 217 StGB. Schneider, Reinhold. Über den Selbstmord (On suicide) (1947). Drei Texte (Three essays), Waltrop/Leipzig 2013. Kruse, Andreas; Maio, Giovanni; Althammer, Jörg. Humanität einer alternden Gesellschaft (Humanity of an ageing society), Paderborn 2014. Kruse, Andreas. Lebensphase hohes Alter. Verletzlichkeit und Reife (Life phase of old age. Vulnerability and maturity), Springer Deutschland 2017. Maio, Giovanni. Den kranken Menschen verstehen (Understanding the sick person), Freiburg/Br. 2015. Bollig, Georg; Heller, Andreas; Völkel, Manuela. Letzte Hilfe. Umsorgen von schwer erkrankten und sterbenden Menschen am Lebensende (Last resource Caring for seriously ill and dying people at the end of life), 2nd edition, Esslingen 2018. Christoph, Franz. Tödlicher Zeitgeist (Deadly zeitgeist), Köln 1980. Hillgruber, Christian. “Die Bedeutung der staatlichen Schutzpflicht für das menschliche Leben und der Garantie der Menschenwürde für eine gesetzliche Regelung der Suizidhilfe” (The importance of the state duty to protect human life and the guarantee of human dignity for a legal regulation of assisted suicide). In: Hoffmann, Thomas; Knaup, Marcus (eds.). Was heisst in Würde sterben. Wider die Normalisierung des Tötens (What does it mean to die with dignity. Against the normalization of killing), Wiesbaden 2015, p. 102–115. Bauer, Axel W. “Notausgang assistierter Suizid? Die Thanatopolitik in Deutschland vor dem Hintergrund des demographischen Wandels” (Emergency exit assisted suicide? The thanato politics in Germany against the background of demographic change). In: Hoffmann, Thomas; Knaup, Marcus (eds.). Was heisst in Würde sterben. Wider die Normalisierung des Tötens (What does it mean to die with dignity. Against the normalization of killing), Wiesbaden 2015, p. 48–78. Beckmann, Rainer; Kaminski, Claudia; Löhr, Mechthild (eds.). Es gibt kein gutes Töten (There is no good killing), Waltrop/Leipzig 2015. Woelki, Rainer Maria Kardinal; Hillgruber, Christian; Maio, Giovanni; von Ritter, Christoph; Spieker, Manfred. Wie wollen wir sterben? (How do we want to die?), Paderborn 2016. Bruns, Theo; Penselin, Ulla, Sierck, Udo (eds.). Tödliche Ethik (Lethal ethics), Hamburg 1990. Bloodworth M., Bloodworth N., Wesley E. “A template for non-religious-based discussions against euthanasia”. In: The Linacre Q. 2015; 82(1), p. 49-54. Sulmasy, D. P.; Travaline, J. M.; Mitchell, L. A.; Ely, E. W. “Non-faith-based arguments against physician-assisted suicide and euthanasia”. In: Linacre Q. 2016; 83(3), p. 246–257
22 Isensee, J. Das Grundrecht auf Sicherheit (The fundamental right to security), Berlin 1983, p. 3
23 Ibid.
24 ibid p. 4
25 ibid p. 5
26 ibid p. 5
27 cf. Mieth, Dietmar. “Sterbehilfe ist nicht zulässig”. (Assisted suicide is not permissible.) In: Rp-online.de,(Interview from 30 July 2008). (https://rp-online.de/leben/gesundheit/news/sterbehilfe-ist-nicht-zulaessig_aid-11621643 (accesssed on 3 March 2019)
28 cf. Flyer Veranstaltungszyklus Autonomie in der Medizin. (Flyer for a series of events on autonomy in medicine.) (www.nek-cne.ch/fileadmin/nek-cne-dateien/Themen/Symposium_NEK-ZEK/NEK-ZEK_2016_Flyer_D.pdf (accessed on 3 December 2016)
29 cf. Hoche, Alfred. Die Freiheit des Willens vom Standpunkte der Psychopathologie. (The freedom of the will from the position of psychopathology.) Wiesbaden 1902, Loewenfeld, L. & Kurella, H. (eds.). Grenzfragen des Nerven- und Seelenlebens. Einzeldarstellungen für Gebildete aller Stände. Band XIV. (Border issues of mental and inner life. Individual presentations for educated people of all classes. Volume XIV.) cf.: “Bilanzsuizid”. (Balanced suicide) In: https://de.wikipedia.org/wiki/Bilanzsuizid#cite_note-1 (accessed on 5 March 2019) cf.: Eser, Albin. “Erscheinungsformen von Suizid und Euthanasie – Ein Typisierungsversuch”. (Manifestations of Suicide and Euthanasia – an approach for typification) In: Eser, Albin (ed.). Suizid und Euthanasie als human- und sozialwissenschaftliches Problem. (Suicide and euthanasia as a human problem and a problem of social science) Stuttgart 1976, pp. 4–11. In 1920, the psychiatrist Alfred Erich Hoche and the lawyer Karl Binding published the brochure “The Extermination of Life Unworthy of Life.” In this text they glorified suicide as “self-determined” death. Additionally, they supported “euthanasia” for the “terminally ill”. And they demanded the killing of sick and disabled people, who they claimed, were only “human shells” and no longer of any value for the society. The brochure was used as a template for the National Socialist “Euthanasia” program.
30 Bochnik, H. J. Suizid und Sterbehilfe. “Zur Frage der freien Willensbestimmung in Verzweiflung”. (Suicide and Euthanasia. On the question of free will in desperation.) In: Psycho 1992;8, p. 736–43. Ernst, Cecil. Exposé zu neueren epidemiologischen Studien zum Suizid. (Exposé on recent epidemiological studies on suicide.) 1999, p. 5. Klesse, Raimund. “Der Todeswunsch aus psychiatrischer Sicht”. (The death wish from a psychiatric perspective) In: Imago Hominis 2003;10(1), p. 37–44. Onkay Ho, A. Suicide: “Rationality and Responsibility for Life”. In: Can J Psychiatry 2014; 59(3), p. 141–7. Leeman, C. P. “Distinguishing among irrational suicide and other forms of hastened death: implications for clinical practice”. In: Psychosomatics 2009; 50 (3), pp. 185–97
31Suizidbeihilfe für alte Menschen. Positionspapier der SGG SFGG SGAP. (Assisted suicide for the elderly. Position paper of the SGG SFGG SGAP). Bern 2014. www.sggssg.ch/cms/media/Positionspapiere/Suizidbeihilfe_Positionspapier_SSGG_SFGG_SGAP_Stand_24-11-2014_def.pdf (accessed on 3 December 2016). Stoppe, G.; Kohn. J.; Schmugge, B.; Suter, E.; Wiesli, U. Positionspapier: Suizidprävention im Alter. (Position paper: Suicide prevention in old age.) www.publichealth.ch/logicio/client/publichealth/file/mental/Positionspapier_Suizidpravention_im_Alter__D_def.pdf (accessed on 3 December 2016). Ruckenbauer, G.; Yazdani, F.; Ravaglia, G. “Suicide in old age: illness or autonomous decision of the will”. In: Arch Geront Geriatr Suppl. 2007;1, pp. 355–358
32 Nestor, Karen et al. “Hilfe beim Sterben, Hilfe zum Sterben oder Hilfe zum Leben?” (Accompaniment of dying patients, assisted suicide, or helping to live?) In: Swiss Medical Forum – Schweizerisches Medizin-Forum 2017;17(35), pp. 738–743, p. 741. cf. Bauer, Axel W. “Notausgang assistierter Suizid? Die Thanato-politik in Deutschland vor dem Hintergrund des demographischen Wandels”. (Emergency exit assisted suicide? Thanato policy in Germany in the light of demographic change.) In: Hoffmann, TS; Knaup, M. Was heisst: In Würde sterben? Wider die Normalisierung des Tötens. (What does it mean to die with dignity? Against the normalisation of killing) Springer. 2015, pp. 49–79; Maio, Giovanni. “Gutes Sterben erfordert mehr als die Respektierung der Autonomie”. (Good dying requires more than respecting autonomy.) In: Deutsche Zeitschrift für Onkologie 2011; 41, pp. 129–132; ibid. “Eine neue Kultur der Sorge am Lebensende”. (A new culture of end-of-life care.) In: pflegen: palliative 22/2014, pp. 8–11; ibid. “Grundelemente einer Care-Ethik”. (Basic elements of a care ethics.) In: Jahrbuch für Recht und Ethik 2016, 24, pp. 241–251; ibid. “Der Krebs als Brennglas des Lebens. Für eine Ethik der Zuwendung in der Onkologie”. (Cancer, as a magnifying of life. For an ethic of care in oncology.) In: Deutsche Zeitschrift für Onkologie 2016, 48; 2, pp. 72–75; Ricoer, Paul. Lebendig bis in den Tod. Fragmente aus dem Nachlass. (Alive until death. Fragments from the estate.) Hamburg, 2011
33 Jones, D. A. & Paton, D. How. “Does Legalization of Physician-Assisted Suicide Affect Rates of Suicide?” In: Southern Medical Journal 2015;108(10), pp. 590–604. Sterbehilfe und Suizid in der Schweiz 2014. (Assisted suicide and suicide in Switzerland 2014) www.bfs.admin.ch/bfs/de/home/statistiken/gesundheit/gesundheitszustand.assetdetail.1023143.html (accessed on 3 December 2016)
34 Ziegler, W. & Hegerl, U. “Der Werther-Effekt”. (The Werther Effect.) In: Nervenarzt 2002;73, pp. 41–49
35 Ziegler W. & Hegerl U. “Der Werther-Effekt”. (The Werther Effect.) In: Nervenarzt 2002;73, pp. 41–49. Scherr, S. & Steinleitner, A. “Zwischen dem Werther- und Papageno-Effekt”. (Between the Werther and Papageno effects.) In: Nervenarzt 2015;86, pp. 557–565. WHO. Preventing suicide. A ressource for medial professionals. www.who.int/mental_health/prevention/suicide/resource_media.pdf (accessed on 3 December 2016)
36 Nestor, Karen et al. “Hilfe beim Sterben, Hilfe zum Sterben oder Hilfe zum Leben?” (Accompaniment of dying patients, assisted suicide, or helping to live?) In: Swiss Medical Forum – Schweizerisches Medizin-Forum 2017;17(35), pp. 738–743, S. 742. Vgl.: Niederkrotenthaler, T.; Voracek, M.; Herberth, A.; Till, B.; Strauss, M.; Etzersdorfer, E. et al. “Role of media reports in completed and prevented suicide: Werther v. Papageno effects”. In: BJ Psych 2010;197, pp. 234–243. ibid: Niederkrotenthaler, T.; Voracek, M.; Herberth, A.; Till, B.; Strauss, M.; Etzersdorfer, E. et al. “Papageno v Werther effect”. In: BMJ 2010;341
Literature
Netherlands
- van der Maas, P. J.; van der Delden, J. J. M.; Pijnenborg, L. Medische beslissingen rond het levenseinde. Het oderzoek voor de Commissie Oderzoek Medische Braktijk inzake Euthanasie. Sdu Uitgrverij Plantijnstraat, ’s-Gravenhage 1991. ISBN 90 39 901244 [= “Remmelink Report”. English translation: Euthanasia and other Medical Decisions Concerning the End of Life. Amsterdam 1992]
- van der Wal, G. & van der Maas, P. J. Euthanasie en andere medische beslissingen rond het levenseinde. Den Haag: SDU 1996
- Hendin, Herbert et al. “Physician-Assisted Suicide and Euthanasia in the Netherlands”. In: Jama, June 4, 1997-Vol 277, No. 21
- Gunning, Karel F. “Euthanasia”. In: The Lancet, 19 October 1991
- Gunning, Karel F. Remmelink and after. London 1992
- Gunning, Karel F. Human rights and Euthanasia in the Netherlands. [Manuscript in the possession of the author: Comparison of official Dutch euthanasia figures from 1990 and 1995]
- Fenigsen, Richard. The Report of the Dutch Government Committee on Euthanasia. Norfolk 1991
- van Raemdonck, D. “Euthanasia patients should be accepted as organ donors in states with existing legislation”. In: Ann Thorac Surg 2016; 102, pp. 1782-1789
- Lerner B. H.; Caplan, A. L. “Euthanasia in Belgium and the Netherlands: On a Slippery Slope?” In: JAMA Intern Med 2015;175(10), pp. 1640–1641
Belgium
- Onwuteaka-Philipsen, B. D.; Brinkman-Stoppelenburg, A.; Penning, C.; de Jong-Krul G. J. F.; van Delden J. J. M.; van der Heide, A.; “Trends in end-of-life practices before and after the enactment of the euthanasia law in the Netherlands from 1990 to 2010: a repeated cross-sectional survey”. In: Lancet 2012; 380, pp. 908–915
- Dierickx, S.; Deliens; L.; Cohen, J.; Chambaere, K.; “Euthanasia in Belgium: trends in reported cases between 2003 and 2013”. In: CMAJ 2016; 188(16), pp. 407–414
- Siegel, A. M.; Sisti, D. A.; Caplan, A. L. “Pediatric Euthanasia in Belgium – Disturbing Developments”. In: JAMA 2014; 311(19), pp. 1963–1964
- “Erstmals Sterbehilfe für todkrankes Kind”. (First euthanasia for terminally ill child.) In: Neue Zürcher Zeitung of 17 September 2016 (https://www.nzz.ch/international/aktuelle-themen/belgien-erster-fall-von-sterbehilfe-fuer-minderjaehrige-ld.117321 (accessed 3 March 2019))
- Ysebaert, D.; van Beeumen, G., de Greef, K.; Squifflet, J. P.; Detry O.; de Roover, A. et al. “Organ procurement after euthanasia: Belgian experience”. In: Transplant Proc 2009;41(2), pp. 585–586
Europe
- van der Heide, A.; Deliens, L.; Faisst, K.; Nilstun, T.; Norup, M.; Paci, E. et al. “End-of-life decision-making in six European countries: descriptive study”. In: Lancet 2003;361, pp. 345–350
Switzerland
- Bosshard, G.; Zellweger, U.; Bopp, M.; Schmid, M.; Hurst, S. A.; Puhan, M. A. et al. “Medical End-of-Life Practices in Switzerland: A Comparison of 2001 and 2013”. In: JAMA Intern Med 2016;176(4), pp. 555–556
- Marti, M. “Sterbehilfe in der Schweiz” (Euthanasia in Switzerland.) In: SAEZ 2002; 83, pp. 570–573
- Tag, Brigitte. “Strafrecht am Ende des Lebens – Sterbehilfe und Hilfe zum Suizid in der Schweiz” (Criminal law at the end of life – euthanasia and assisted suicide in Switzerland.) In: ZSTW 2016;128(1), pp. 73–88

(Picture mn)
M.A. and lic. phil. Moritz Nestor: Studies in German and philosophy (Freiburg i.B., Germany) and psychology and educational Sciences Zurich; postgraduate training in psychotherapy as well as complementary studies in adult psychopathology. He worked for many years as a teacher of German as a foreign language, and today as a psychologist in private practice.
Editor of Forum “Naturrecht und Humanismus” (Natural law and Humanism) (www.naturrecht.ch); editor of the journal “Personale Psychologie und Pädagogik” (Personalist Psychology and Pedagogy); founding and board member of the “Hippokratische Gesellschaft Schweiz” (Hippocratic Society Switzerland); founding and board member of the “Institut für Personale Humanwissenschaften und Gesellschaftsfragen, IPHG” (Institute for the Personal Humanities and Social Issues, IPHSI); extensive lecturing and publishing activity.
Upholding human dignity – until the last breath
by Erika Vögeli
It is a great achievement of the Thurgau Church to have presented with a project and a resulting publication a positive alternative to the highly publicised discussion about assisted suicide and the accompanying – mostly unspoken – dangerous shift in emphasis in the attitude towards human life. It places dignity, self-determination and autonomy, but also compassion for the suffering, in the social context without which these concepts have no real meaning. Even if we recognise it as inalienable and inviolable, the experience of our dignity always has a social reference and always depends on how we experience ourselves in the encounter with our fellow human beings. It is not the increase in the need for help that touches it, but, as the blurb states, the “tendency of society that calls into question the inalienable dignity of vulnerable life.”
Talking about end of life and dying is difficult for most people and associated with various emotions. Fears, feelings of insecurity, ambiguities due to current discussions about self-determination and dignity in these questions preoccupy many. Sometimes predictably, often abruptly we are – being sick or suffering or as relatives – confronted with questions that are complex and burden us because they affect the core of our being. How long should life-prolonging measures be maintained? When can it make sense to withhold therapy and what does that mean? What do dignity and self-determination mean in this context? A loved one says he or she wants to die – what does that mean?
The Protestant Church of the canton of Thurgau has answered such questions with the publication “Den Weg zu Ende gehen. In der Begegnung mit dem Sterben Lebendigkeit erfahren” (Walking the path to the end. Experiencing aliveness in the encounter with dying.) It is a beautifully designed handout that makes the experiences and thoughts of experts from various disciplines (theology, medicine, jurisprudence, gerontology) and of relatives accessible to those affected and anyone interested, and provides valuable suggestions.
The editors are concerned with an attitude “which does not want to condemn those who bear the thought of a possible suicide, but which is clearly directed against a tendency of society which calls into question the inalienable dignity of vulnerable life” (blurb). And in their introductory statement they also warn of the far-reaching consequences for the individual as well as for society as a whole if suicide “even outside of the greatest personal emergencies was to become a normal end-of-life option.” It would be an “epochal change in the view of life” with “far-reaching consequences for many areas of life.” (pp. 15)
The considerations presented in the book are not solely religiously based; in their fundamental nature, in their ethical and anthropological reference, they are just as relevant to every secularly oriented person. The fact that “there is a God above man”, as the editors write with reference to Dietrich Bonhoeffer, also points to the fact that we as humans cannot create life. Even if such fantasies of omnipotence and ideas of feasibility do circulate. The same applies to the statement that living and dying always have something to do with our fellow human beings: “From birth, we are not people simply living for ourselves alone and responsible only to ourselves, this we are not even after we have attained our majority, and we are not even when we die.” (p. 15) And it also applies to the statement that “an essential aspect of the life and self-understanding of Christians is that we care for one another.”
Important legal considerations on the patient’s self-determination and responsibility for his own decisions also belong in this context. “Of course, a doctor should not be allowed to decide over the patient’s head,” (p. 21). But placing the responsibility for medical treatment at the end of life on the patient or on his or her aged spouse can become a serious imposition. “The over-emphasis on patient autonomy runs the risk of turning against the person concerned and placing only one-sided responsibility on them, rather than providing them with the care and companionship they need.” (p. 24)
All contributions emphasise the importance of human relationships and the fact that absolute autonomy does not exist. We all need a social network, not only the sick and the dying – but the latter, by nature, to a special degree. This is also the basic idea of palliative nursing and care: to show its possibilities and importance and to anchor the knowledge about it as broadly as possible in the population, is therefore also a central concern of the publication, which is expressed in all contributions. Time and again, it is also discussed that we need to reflect on the fact that dignity must not only be linked to performance and efficiency, but also belongs to the human being in the case of decreasing strength, increasing weakness and need for help. “However, it must be possible to experience the dignity of a person.” – in trusting, living, social relationships, according to one of the authors. (p. 54)
Thus, it is also addressed that autonomy and self-determination take place in the social context, and the question of assisted suicide always includes the counterpart of the person in need. This second person has to decide whether to try to “give value back to him or her, to show him or her new perspectives in dealing with a difficult situation, to endure the difficult situation with him or her” or to share the assessment that this life is no longer worth living. Thus, the attitude of this other person “will always influence the suicide wish in one direction or another – self-determination does not release any fellow human being, and certainly not a doctor, from responsibility.” (p.82) The killing itself – or witnessing an assisted suicide – leads to psychological injuries, for example in the form of post-traumatic stress disorders and depression. Conversely, experiencing “how people overcome crisis situations with the help of their fellow human beings and go through developments” gives everyone courage and hope. (p. 84)
The descriptions of a family doctor are also touching and lead the way in this regard: His experiences show impressively that even in people who place great value on self-determination and independence, the desire for assisted suicide is silenced when they feel supported in a human relationship. This includes talking about the possibilities of palliative care and support in the terminal phase in the personal environment. This has nothing to do with the much-discussed unnecessary prolongation of life by monstrous machines (a false idea that is outdated anyway) – here it is about a procedure that is completely tailored to the patient and developed with him or her, which allows him or her to become calm with as little pain as possible, to let go inwardly and to fall asleep peacefully.
The fact that this is a very different experience also for the relatives than a possible assisted suicide is proven by the equally touching testimonials of people who have accompanied a close relative in the last phase. They “hold a deep treasure of experience” as the blurb rightly puts it. They tell of challenging times with highs and lows, but also of gratitude for the time given together, of new experiences and reconciliation, of strengthened family cohesion and the encouraging certainty of having overcome even this life situation together.
A publication that invites reflection and encourages us, in the debate about self-determination and dignity at the end of life, not to lose sight of the fact that the vulnerability of all human life is part of our existence – if we reject it, we also violate the humanity within ourselves. But first and foremost a reading that brings us closer to the subject in a way that is humanly unifying and encouraging. We wish it numerous readers.